
Thyroid Surgery
GENERAL INFORMATION
Your doctor may recommend that you consider thyroid surgery for 4 main reasons:
- You have a nodule that might be thyroid cancer.
- You have a diagnosis of thyroid cancer.
- You have a nodule or goiter that is causing local symptoms – compression of the trachea, difficulty swallowing or a visible or unsightly mass.
- You have a nodule or goiter that is causing symptoms due to the production and release of excess thyroid hormone – either a toxic nodule, a toxic multinodular goiter or Graves’ disease.
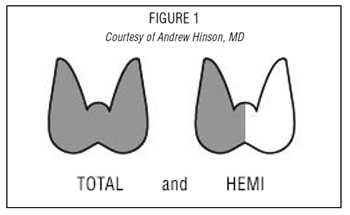
The extent of your thyroid surgery should be discussed by you and your thyroid surgeon and can generally be classified as a partial thyroidectomy or a total thyroidectomy. Removal of part of the thyroid can be classified as:
- An open thyroid biopsy – a rarely used operation where a nodule is excised directly;
- A hemi-thyroidectomy or thyroid lobectomy – where one lobe (one half) of the thyroid is removed;
- An isthmusectomy – removal of just the bridge of thyroid tissue between the two lobes; used specifically for small tumors that are located in the isthmus.
- Finally, a total or near-total thyroidectomy is removal of all or most of the thyroid tissue. (Figure 1)
The recommendation as to the extent of thyroid surgery will be determined by the reason for the surgery. For instance, a nodule confined to one side of the thyroid may be treated with a hemithyroidectomy. If you are being evaluated for a large bilateral goiter or a large thyroid cancer, then you will probably have a recommendation for a total thyroidectomy. However, the extent of surgery is both a complex medical decision as well as a complex personal decision and should be made in conjunction with your endocrinologist and surgeon.
Thyroid Surgery FAQs
QUESTIONS AND CONSIDERATIONS
When thyroid surgery is recommended, patients should ask several questions regarding the surgery including:
- Why do I need an operation?
- Are there other forms of treatment?
- How should I be evaluated prior to the operation?
- How do I select a surgeon?
- What are the risks of the operation?
- How much of my thyroid gland needs to be removed?
- Will I need to take a thyroid pill after my operation?
- What can I expect once I decide to proceed with surgery?
- What will be my physical restrictions following surgery?
- Will I lead a normal life after surgery?
WHY DO I NEED AN OPERATION?
The most common reason for thyroid surgery is to remove a thyroid nodule, which has been found to be suspicious through a fine needle aspiration biopsy (see Thyroid Nodule brochure). Surgery may be recommended for the following biopsy results:
- cancer (papillary cancer);
- possible cancer (follicular neoplasm or atypical findings); or
- inconclusive biopsy;
- molecular marker testing of biopsy specimen which indicates a risk for malignancy.
Surgery may be also recommended for nodules with benign biopsy results if the nodule is large, if it continues to increase in size or if it is causing symptoms (discomfort, difficulty swallowing, etc.). Surgery is also an option for the treatment of hyperthyroidism (Grave’s disease or a “toxic nodule” (see Hyperthyroidism brochure), for large and multinodular goiters and for any goiter that may be causing symptoms.
ARE THERE OTHER MEANS OF TREATMENT?
Surgery is definitely indicated to remove nodules suspicious for thyroid cancer. In the absence of a possibility of thyroid cancer, there may be nonsurgical options for therapy depending on your diagnosis. You should discuss other options for treatment with your physician who has expertise in thyroid diseases.
HOW SHOULD I BE EVALUATED PRIOR TO THE OPERATION?
As for other operations, all patients considering thyroid surgery should be evaluated preoperatively with a thorough and detailed medical history and physical exam including cardiopulmonary (heart and lungs) evaluation. An electrocardiogram and a chest x-ray prior to surgery are often recommended for patients who are over 45 years of age or who are symptomatic from heart disease. Blood tests may be performed to determine if a bleeding disorder is present.
Importantly, any patient who has had a change in voice or who has had a previous neck operation (thyroid surgery, parathyroid surgery, spine surgery, carotid artery surgery, etc.) and/or who has had a suspected invasive thyroid cancer should have their vocal cord function evaluated routinely before surgery. This is necessary to determine whether the recurrent laryngeal nerves that control the vocal cord muscles are functioning normally.
Finally, in rare cases, if medullary thyroid cancer is suspected, patients should be evaluated for endocrine tumors that occur as part of familial syndromes including adrenal tumors (pheochromocytomas) and enlarged parathyroid glands that produce excess parathyroid hormone (hyperparathyroidism).
HOW DO I SELECT A SURGEON?
In general, thyroid surgery is best performed by a surgeon who has received special training and who performs thyroid surgery on a regular basis. The complication rate of thyroid operations is lower when the operation is done by a surgeon who does a large number of thyroid operations each year. Patients should ask their referring physician where he or she would go to have a thyroid operation or where he or she would send a family member.
WHAT ARE THE RISKS OF THE OPERATION?
In experienced hands, thyroid surgery is generally very safe. Complications are uncommon, but the most serious possible risks of thyroid surgery include:
- bleeding in the hours right after surgery that could lead to acute respiratory distress;
- injury to a recurrent laryngeal nerve that can cause temporary or permanent hoarseness, and possibly even acute respiratory distress in the very rare event that both nerves are injured;
- damage to the parathyroid glands that control calcium levels in the blood, leading to temporary, or more rarely, permanent hypoparathyroidism and hypocalcemia.
These complications occur more frequently in patients with invasive tumors or extensive lymph node involvement, in patients undergoing a second thyroid surgery, and in patients with large goiters that go below the collarbone into the top of the chest (substernal goiter). Overall the risk of any serious complication should be less than 2%. However, the risk of complications discussed with the patient should be the particular surgeon’s risks rather than that quoted in the literature. Prior to surgery, patients should understand the reasons for the operation, the alternative methods of treatment, and the potential risks and benefits of the operation (informed consent).
HOW MUCH OF MY THYROID GLAND NEEDS TO BE REMOVED?
Your surgeon should explain the planned thyroid operation, such as lobectomy (hemi) or total thyroidectomy, and the reasons why such a procedure is recommended.
For patients with papillary or follicular thyroid cancer, many, but not all, surgeons recommend total or neartotal thyroidectomy when they believe that subsequent treatment with radioactive iodine might be necessary. For patients with larger (>1.5 cm) or more invasive cancers and for patients with medullary thyroid cancer, local lymph node dissection may be necessary to remove possibly involved lymph node metastases.
A hemithyroidectomy may be recommended for overactive solitary nodules or for benign onesided nodules that are causing local symptoms such as compression, hoarseness, shortness of breath or difficulty swallowing. A total or near – total thyroidectomy may be recommended for patients with Graves’ Disease (see Hyperthyroidism brochure) or for patients with large multinodular goiters.
WILL I NEED TO TAKE A THYROID PILL AFTER MY OPERATION?
The answer to this depends on how much of the thyroid gland is removed. If half (hemi) thyroidectomy is performed, there is an 80% chance you will not require a thyroid pill UNLESS you are already on thyroid medication for low thyroid hormone levels (e.g. Hashimoto’s thyroiditis) or have evidence that your thyroid function is on the lower side in your thyroid blood tests. If you have your entire gland removed (total thyroidectomy) or if you have had prior thyroid surgery and now are facing removal of the remaining thyroid (completion thyroidectomy) then you have no internal source of thyroid hormone remaining and you will definitely need lifelong thyroid hormone replacement.
WHAT CAN I EXPECT ONCE I DECIDE TO PROCEED WITH SURGERY?
Once you have met with the surgeon and decided to proceed with surgery, you will be scheduled for your pre-operative evaluation (see above) You should have nothing to eat or drink after midnight on the day before surgery and should leave valuables and jewelry at home.
The surgery usually takes 2-2½ hours, after which time you will slowly wake up in the recovery room. Surgery may be performed through a standard incision in the neck or may be done through a smaller incision with the aid of a video camera (Minimally invasive video assisted thyroidectomy). Under special circumstances, thyroid surgery can be performed with the assistance of a robot through a distant incision in either the axilla or the back of the neck. There may be a surgical drain in the incision in your neck (which will be removed after the surgery) and your throat may be sore because of the breathing tube placed during the operation. Once you are fully awake, you will be allowed to have something light to eat and drink. Many patients having thyroid operations, especially after hemithyroidectomy, are able to go home the same day after a period of observation in the hospital. Some patients will be admitted to the hospital overnight and discharged the next morning.
WHAT WILL BE MY PHYSICAL RESTRICTIONS FOLLOWING SURGERY?
Most surgeons prefer that patients limit extreme physical activities following surgery for a few days or weeks. This is primarily to reduce the risk of a postoperative neck hematoma (blood clot) and breaking of stitches in the wound closure. These limitations are brief, usually followed by a quick transition back to unrestricted activity. Normal activity can begin on the first postoperative day. Vigorous sports, such as swimming, and activities that include heavy lifting should be delayed for at least ten days to 2 weeks.
WILL I BE ABLE TO LEAD A NORMAL LIFE AFTER SURGERY?
Yes. Once you have recovered from the effects of thyroid surgery, you will usually be able to do anything that you could do prior to surgery. Some patients become hypothyroid following thyroid surgery, requiring treatment with thyroid hormone (see Hypothyroidism brochure). This is especially true if you had your whole thyroid gland removed. Generally, you will be started on thyroid hormone the day after surgery, even if there are plans for treatment with radioactive iodine.

 Printable Brochures
Printable Brochures
Articles
Thyroid Health Blog: Parathyroid Glands – Why and how we should preserve them during neck surgery
FURTHER INFORMATION
For information on thyroid patient support organizations, please visit the Patient Support Links section on the ATA website at www.thyroid.org

