
Adult Hypothyroidism
WHAT IS HYPOTHYROIDISM?
Hypothyroidism happens when the thyroid doesn’t make enough hormones.
Hypothyroidism FAQS
WHAT IS THE THYROID GLAND?
The thyroid gland is a butterfly-shaped endocrine gland that is normally located in the lower front of the neck. The thyroid’s job is to make thyroid hormones, which are released into the blood and then carried to every tissue in the body. Thyroid hormone helps the body use energy, control metabolism, stay warm and help the brain, heart, muscles, and other organs working as they should.
WHAT ARE THE SYMPTOMS?
If your thyroid hormone levels are low, your body slows down. You may:
- Feel cold
- Feel tired
- Have dry skin
- Be constipated
- Feel sad or down
- Forget things easily
Not everyone has all these symptoms, and other health problems can cause them too. A blood test is the only way to know for sure if you have hypothyroidism.
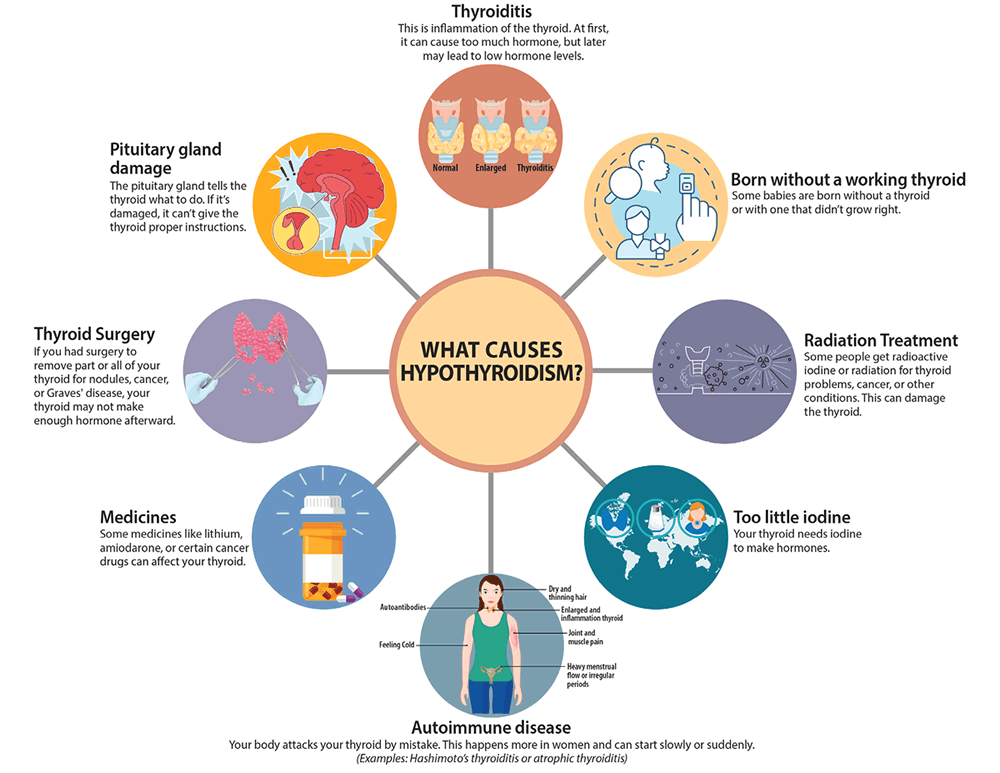
WHAT CAUSES HYPOTHYROIDISM?
There are many reasons why your thyroid might not make enough hormones:
- Autoimmune disease. Your body attacks your thyroid by mistake. This happens more in women and can start slowly or suddenly. (Examples: Hashimoto’s thyroiditis or atrophic thyroiditis)
- Thyroid surgery. If you had surgery to remove part or all of your thyroid for nodules, cancer, or Graves’ disease, your thyroid may not make enough hormone afterward.
- Radiation treatment. Some people get radioactive iodine or radiation for thyroid problems, cancer, or other conditions. This can damage the thyroid.
- Born without a working thyroid. Some babies are born without a thyroid or with one that didn’t grow right.
- Thyroiditis. This is inflammation of the thyroid. At first, it can cause too much hormone but later may lead to low hormone levels.
- Medicines. Some medicines like lithium, amiodarone, or certain cancer drugs can affect your thyroid.
- Too little iodine. Your thyroid needs iodine to make hormones.
- Pituitary gland damage. The pituitary gland tells the thyroid what to do. If it’s damaged, it can’t give the thyroid proper instructions.
HOW IS HYPOTHYROIDISM DIAGNOSED?
Doctors use two main blood tests:
- TSH Test. TSH is a hormone from the pituitary gland that tells the thyroid to work. If your thyroid is not making enough hormone, your TSH goes up. But if the pituitary is damaged, this test may not help.
- Free T4 Test. This test checks the amount of thyroid hormone in your blood that your body can actually use. Testing for the T3 hormone is not often needed. Most of the T3 in your body comes from T4, and it doesn’t help much in diagnosing hypothyroidism.
HOW IS HYPOTHYROIDISM TREATED?
You take a thyroid hormone pill every day. This medicine is called levothyroxine or T4. Some people need a supplemental dose to add to what their thyroid produces while others take a replacement dose because their thyroid doesn’t produce any thyroid hormone.
Sometimes people may also need a second medicine called liothyronine or T3 if they don’t feel better with T4 alone.
SIDE EFFECTS AND COMPLICATIONS
Taking too much or too little medicine can cause problems.
Too little: You may still feel tired, cold, or constipated.
Too much: You may feel nervous, have a fast heartbeat, feel hot, or lose weight.
If you feel these symptoms, tell your doctor. You may need to change your dose.
FOLLOW-UP
Your doctor will check your blood 6 to 8 weeks after starting or changing your thyroid hormone dose. If you’re pregnant or take other medicines, you may need more frequent checks.
Babies with hypothyroidism need regular checks as they grow.
WHAT TO EXPECT LONG-TERM
Most people take thyroid medicine for life. But if your thyroid problem came from a virus or happened after pregnancy, it may go away.
Your dose may change over time. With the right dose, you can live a normal, healthy life.
WHEN TO SEE YOUR DOCTOR
- Call your doctor if:
- Your symptoms come back or get worse
- You want to change your dose, brand, or how you take your medicine
- You gain or lose a lot of weight (10 pounds or more)
- You start or stop taking a medicine that affects thyroid pills, like:
- Antacids
- Calcium or iron supplements
- Biotin
- Estrogen (like in birth control)
- Seizure medicine (phenytoin, Tegretol)
- You miss doses – be honest about it. It’s safe to make up the missed dose by taking a double dose the next day.
- You want to stop taking thyroid medicine (only do this with your doctor’s help)
- You are planning to get pregnant or are already pregnant
LET OTHERS KNOW
Tell your other doctors and your pharmacist about your thyroid condition. Since thyroid problems can run in families, tell your family too.

Articles
Can Vitamin D supplementation prevent autoimmune thyroid disease leading to hypothyroidism? – Clinical Thyroidology® for the Public
FURTHER INFORMATION
For information on thyroid patient support organizations, please visit the Patient Support Links section on the ATA website at www.thyroid.org
